





Melanoma is a cancer of the skin. So what causes skin cancer?
Ultraviolet Radiation (UV) is the main risk factor for skin cancers. Too much exposure to ultraviolet (UV) radiation can damage the genetic material (DNA) in your skin cells and cause skin cancer. The sun naturally gives out UV, whilst the UV from sunbeds is artificial.
UV radiation is divided by wavelength into 3 types: UVA, UVB and UVC.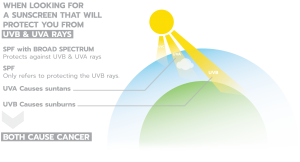
UVC has the shortest wavelength and is the most powerful and potentially harmful; but UVC rays are absorbed in the ozone and don’t make it to the surface of the planet in large enough doses to have an impact on our skin.
UVA and UVB are a different story, though. Both make it through the atmosphere intact, and both can be harmful to your skin, including increasing your risk of developing skin cancer.
Both types can cause skin cancer:
- UVB is responsible for the majority of sunburns.
- UVA penetrates deep into the skin. It ages the skin but contributes much less towards sunburn.
You can’t feel UV rays – the heat from the sun comes from infrared rays, which can’t burn you. This is why people can still burn on cool days.
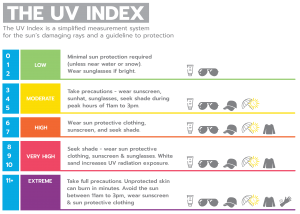
The UV Index is a scale that was developed by the World Health Organisation and measures the level of UV from the sun at the surface, the higher the UV index the greater the risk of skin damage. When the UV index is 3 or above you need to protect your skin.
About Our New Skin Cancer Treatment
We are delighted to give the green light to an exciting new skin cancer research project this July. The novel treatment for skin cancers uses a technique called Electroporation in combination with calcium replacing of the existing combination of this technology with chemotherapy that has been available in Cork since the early 2000s. It is hoped that this new treatment could be available for patients in a clinical trial as early as November.
This builds on the many years supporters of Breakthrough Cancer Research have helped fund research on the use of Electrochemotherapy to treat skin cancers including Basal Cell Carcinomas (BCCs), Squamous Cell Carcinomas (SCCs) & Melanoma.
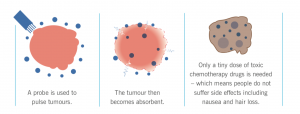
Electrochemotherapy (ECT) is a localised treatment technique where cells are temporarily permeabilized after exposure to a brief electrical pulse and combined with low dose chemotherapy to ablate malignancies. It is a technique causing minimal damage to the surrounding healthy tissue and has the potential to avoid the need for complex reconstruction. The role of ECT as a primary treatment modality is still being investigated but it is an established treatment for skin metastases.
In one Breakthrough Cancer Research funded randomised controlled trial investigating whether Electrochemotherapy could be effectively used as a primary treatment for Basal Cell carcinoma (BCC), the most common skin cancer. Patients were followed for 5 years. In the ECT group, 86% had complete response at 60 days. 11% had a second treatment following which 100% complete response was observed and did not return after 5 years of follow up.
The authors, led by surgeon, Mr Jim Clover, concluded that this study, the first randomised controlled trial of its kind, confirmed that ECT is an effect treatment for BCC, with good long term treatment response.
The complete study is available at the following link: https://doi.org/10.1016/j.ejso.2019.11.509
There is a need to continue to expand the therapeutic toolbox to increase more effective and less invasive treatment options for patients that are unsuitable for or unwilling to undergo the current therapies.
Electrochemotherapy is a targeted treatment, which reduces the use of toxic chemotherapy drugs to a minimal level. It is now hoped to continue this research using Calcium electroporation as a novel anti-cancer treatment where lethally high calcium concentrations are introduced into the cancer cells by electroporation. The usage of calcium instead of chemotherapeutic drugs presents several potential advantages including no damage to the surrounding tissue, long durability, medical professionals other than oncologists can administer it, and once electrodes and electroporator are in place, it is inexpensive.
This research will build on research with collaborators in Denmark who have been looking at the use of electroporation delivered in an outpatient setting with local anaesthetic and in combination with calcium. They have been also investigating the immune engagement resulting from electroporation and calcium treatment.


 Contact
Contact